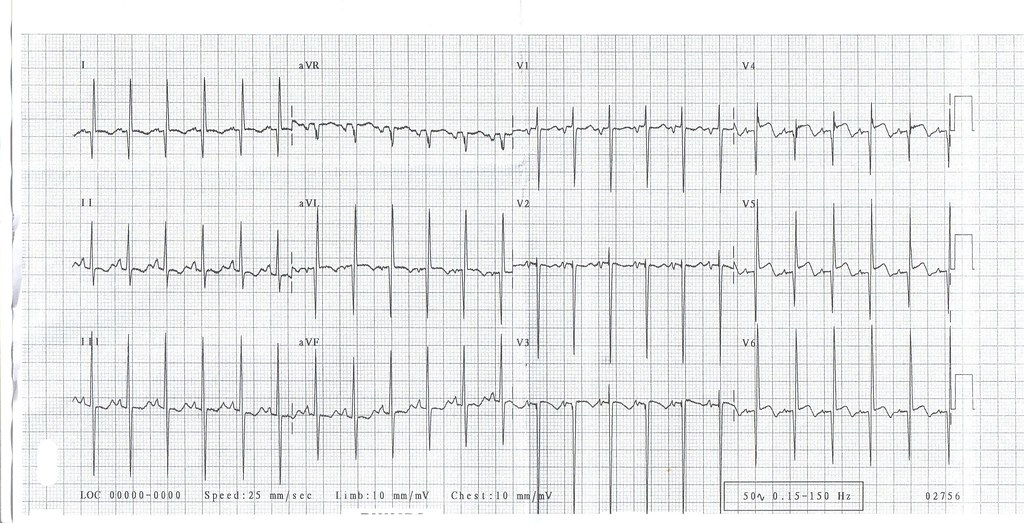
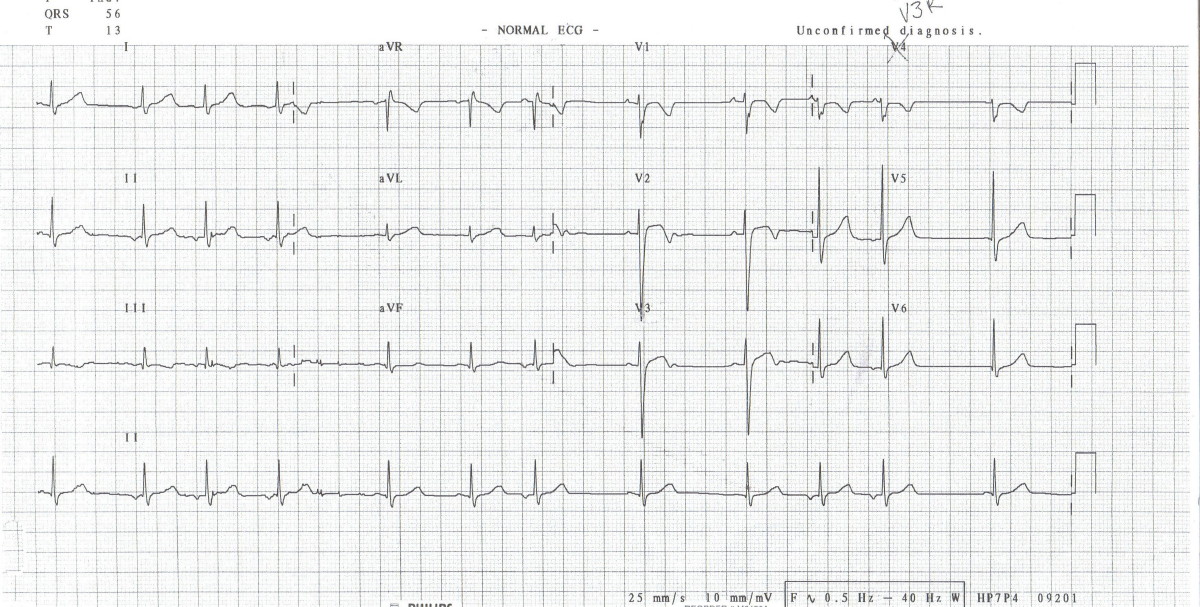
A 5 years old boy with Atrial Septal Defect attended for pre-operative medical examination. He had a irregular pulse. Attached is the ECG of this child.
1. What is the diagnosis?
A) Sinus arrhythmia
B) Wandering Atrial Pacemaker
C) Atrial Fibrilation
D) Complete Heart Block
E) Second Degree Heart Block
2. What is the significance of this finding?
A) no clinical significance
B) This child is at risk of sudden death from cardiac arrhythmias
C) This child is in cardiac failure
D) This child needs a permanent cardiac pacemaker implantation
E) This child needs anticoagulation